Ficheiro:Male suicide rates 2015 (crude).svg

Imagem numa resolução maior (ficheiro SVG, de 512 × 231 píxeis, tamanho: 1,25 MB)
|
|
Esta imagem provém do Wikimedia Commons, um acervo de conteúdo livre da Wikimedia Foundation que pode ser utilizado por outros projetos.
|
Descrição do ficheiro
| Descrição |
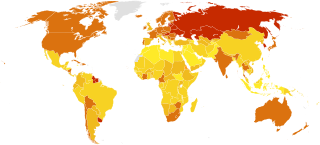
English: Suicide rates per 100,000 males in 2015. Data by World Health Organization (rev. April 2018).
No data
0 - 5
5 - 10
10 - 15
15 - 30
Above 30
Gender differences in suicide are described since the 1990s, by traditionally higher male suicide rates as contraposed to a typical disproportion of females in nonfatal suicide behavior; a relevant review of previous years' data later mentioned throughout the 2000s, noted this male/female disproportion in suicidality throughout Western countries: the proportion of male suicides was incongruous with that of female suicide attempts, as the male-female ratio of suicides was above 2.4 meaning males completed suicide at least 140% more than females, while the female-male ratio of suicide attempts was 1.5 meaning females attempted suicide 50% more than males. Global average was 1.9 in year 2012 according to the WHO, and 2.0 according to the IHME.[1][2][3] Mortality data is always estimated at a degree. Cited as 'gender paradox of suicidal behavior', it is essentially attributed to post-industrial sociocultural influences and gendered identities: females being more vulnerable to psychological problems and receptive to psychotherapeutic approaches (in western societies mental-health disorders are 20-40% higher in women than men, and female therapists outnumber male) particularly at a young age, report suicide ideation and attempt more frequently and are allowed to discuss their emotions, but males being required to express strength and stoicism assuming social status and working roles crucial for their identity are less likely to seek help for suicidal feelings. Since nonfatal suicidal behavior is typically higher in females while suicide rates are traditionally higher for males, then male vulnerability to suicidal behavior is often explained in terms of higher lethality of suicide methods used and hopelessness, being nevertheless that stigmatization of suicidal behaviors tends to frame surviving a suicidal act and seeking help for mental distress as something ‘inappropriate’ for men: research suggests that the gender gap is partially a result of the choice of more lethal methods and the experience of more aggression, which rather provide an indication of the higher intent to die in men.[4][5][6][7] This gender gap holds true in western cultures, while narrows elsewhere, unto where these patterns are contradicted entirely in various Asian societies (counting almost half of global population). Indeed gender differences in suicide vary significantly among countries: western societies (cultural heritage of european origin, such as european languages or religion) report a higher male mortality by suicide than any other, while South and East Asian a much lower, with China accounting for the greatest number of female suicides.  Wealth is also a constant, being that the gender gap is generally limited or non-existent in low- and middle-income societies, whereas it is never absent in high-income countries (depicted in darker green aside): 200,000 deliberately take their own life in Europe and the Americas every year, about 40,000 females and 150,000 males.[8][9][10] The problem then is not the old-fashioned question — why do so many women commit suicide in China; the actual question is why do so many men commit suicide in high-income countries?[11] In the last 45 years suicide rates have increased by 60% worldwide. An estimated one million people per year die by suicide or a death every 40 seconds or about 3,000 every day (more people die from suicide than from murder and war). At the same time, nonfatal episodes are reported up to 20 times as much, with female adolescents and minority groups (migrants, transgenders, etc.) bearing most relevant socio-economic implications for suicide prevention.[12][13][14]
Late 1890s recorded first gender-related observation on suicide by Émile Durkheim: according to statistics of the time, more men died of suicide than women every year. Also, Durkheim mentioned relations between western industrialization, modern communities and vulnerability to self-destructive behavior, suggesting social norms and pressures have effects on suicide.[10][19] Reinforcement of male gender roles such as strength, independence, risk-taking behavior, often prevents males from seeking help for suicidal feelings and depression.[20][21] It is observed that shifting cultural attitudes about gender roles and social norms and especially ideas about masculinity, may also contribute to closing the gender gap.[5][7][22] Suicidal behavior is also subject of study for economists since about the 1970s: although national costs of suicide and suicide attempts (up to 20 for every one completed suicide) are very high, suicide prevention is hampered by scarce resources for lack of interest by mental health advocates and legislators; and moreover, personal interests even financial are studied with regards to suicide attempts for example, in which insights are given that often "individuals contemplating suicide do not just choose between life and death [..] the resulting formula contains a somewhat paradoxical conclusion: attempting suicide can be a rational choice, but only if there is a high likelihood it will cause the attempter's life to significantly improve."[23][24] In the United States alone, yearly costs of suicide and suicide attempts are comprised in 50-100 billion dollars.[25][26]
Social stigma is considered as well a "major barrier" to suicide prevention, and "the underlying motive for discrimination [..] caused by lack of knowledge - ignorance [..] One extreme example is the criminalization of suicidal behaviour, which still occurs in many countries."[28][29] Per recent releases, the World Health Organization warns about social stigma towards suicidal behavior and psychiatric patients, and the taboo to openly discuss suicide, representing to date challenges and obstacles for suicide prevention policies along with low availability and quality of data.[27]
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Data | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Origem |
Based on
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Autor | multiple | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Outras versões |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SVG desenvolvimento | O código-fonte desta imagem SVG é válido. Este(a) desenho vetorial foi criado com o Inkscape, ou com outro programa. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
.svg)
.svg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.svg){kind=link}
{kind=link}
{kind=link}
Licenciamento
| A utilização deste ficheiro é regulada nos termos Creative Commons - CC0 1.0 Dedicação Universal ao Domínio Público. | |
| A pessoa que associou uma obra a este documento dedicou-a ao domínio público, renunciando a todos os seus direitos sobre a obra em todo o mundo ao abrigo da legislação de direitos de autor, incluindo a todos os direitos legais conexos, na medida permitida por lei. Pode copiar, modificar, distribuir e executar a obra, até com fins comerciais, sem pedir autorização.
|
| Eu, titular dos direitos de autor desta obra, dedico-a ao domínio público, com aplicação em todo o mundo. Nalguns países isto pode não ser legalmente possível; se assim for: Concedo a todos o direito de usar esta obra para qualquer fim, sem quaisquer condições, a menos que tais condições sejam impostas por lei. |
Histórico do ficheiro
Clique uma data e hora para ver o ficheiro tal como ele se encontrava nessa altura.
| Data e hora | Miniatura | Dimensões | Utilizador | Comentário | |
|---|---|---|---|---|---|
| atual | 16h42min de 22 de dezembro de 2018 | | 512 × 231 (1,25 MB) | SuperSucker | fix - red (5th color) was wrong |
| 16h11min de 22 de dezembro de 2018 |  | 512 × 231 (1,25 MB) | SuperSucker | fix - brighter yellow (using R-G-B units of 7-24-5 (instead of 7-23-5) | |
| 23h57min de 21 de dezembro de 2018 |  | 512 × 231 (1,25 MB) | SuperSucker | fix - better color homogeneity and appropriateness: this proportioning is based on the R-G-B values (units of 7-23-5 respectively) | |
| 18h02min de 19 de dezembro de 2018 |  | 512 × 231 (1,25 MB) | SuperSucker | fix - removed width and height parameters so it automatically resizes to fit the display | |
| 04h05min de 3 de dezembro de 2018 |  | 2 500 × 1 130 (1,25 MB) | SuperSucker | fix - better intervals (five instead of six) and shades | |
| 02h39min de 27 de outubro de 2018 |  | 2 500 × 1 130 (1,25 MB) | SuperSucker | lighter shades for <15 rates | |
| 19h59min de 22 de outubro de 2018 |  | 2 500 × 1 130 (1,25 MB) | SuperSucker | cleaned up superfluous svg instructions for an overall lighter file | |
| 21h52min de 29 de agosto de 2018 |  | 2 500 × 1 130 (1,34 MB) | SuperSucker | User created page with UploadWizard |
Utilização local do ficheiro
A seguinte página usa este ficheiro:
Utilização global do ficheiro
As seguintes wikis usam este ficheiro:
- ar.wikipedia.org
- as.wikipedia.org
- ca.wikipedia.org
- en.wikipedia.org
- fi.wikipedia.org
.svg){kind=link}